One of the most common questions we hear at Dubai Podiatry Centre is: “Why won’t my nail fungus clear, even though I’ve tried home remedies?”
The answer is that not all fungal nail infections are the same.
Different types of nail fungus affect different parts of the toenail, and each type requires a different treatment approach. This is why a treatment that works for one person may have little or no effect for another.

Superficial White Nail Fungus
One of the easiest types of fungal infection to treat is superficial white fungal infection.
This commonly develops in warm, humid conditions inside closed footwear and under nail polish. The fungus affects only the surface of the nail and often appears as white, chalky or powdery patches on the top of the toenail.
Because the infection is only on the surface, the affected layer can often be gently reduced with professional nail filing or careful buffing, allowing a topical antifungal nail lacquer to reach the remaining fungus more effectively.
As the nail gradually grows out, the healthy nail replaces the infected portion.
Fungus Growing Beneath the Nail
A more difficult type of fungal infection develops underneath the nail plate.
This is commonly associated with a widespread fungal skin infection affecting the sole of the foot, often referred to as moccasin-type athlete’s foot. The fungus can spread beneath the toenail, where it becomes protected by the thick nail plate.
When the fungus is trapped underneath the nail, simply painting antifungal medication onto the surface often has limited success because the medication cannot adequately reach the infection.
Depending on the severity of the infection, treatment may involve oral antifungal medication, careful reduction of the thickened nail, or, in selected cases, nail avulsion of the toenail to allow direct treatment of the underlying nail bed as the new nail grows.
Following nail removal, the smaller toenails generally regrow in approximately three months, while the big toenail may take anywhere from six months to one year to fully regrow.
Fungus That Reaches the Nail Root
In some patients, the fungal infection extends into the nail root (matrix), where the nail is produced.
When this occurs, oral antifungal medication is often recommended because the medication reaches the growing nail through the bloodstream, allowing the new nail to grow free of infection.
If there is also extensive fungal material trapped beneath a thick or damaged nail plate, reducing or removing the affected nail may be recommended to improve access for topical treatment and encourage healthy nail regrowth.
When Oral Medication Is Not Suitable
Before prescribing oral antifungal medication, liver function blood tests are often performed to ensure the medication can be taken safely.
Occasionally, these tests identify previously undiagnosed liver abnormalities. In these situations, even patients who feel completely healthy may not be suitable candidates for oral antifungal medication.
For these patients, treatment may focus on physical methods, including removal of the infected toenail where appropriate, combined with topical antifungal medication applied directly to the exposed nail bed after healing. This allows the new nail to grow in an environment with a much lower fungal burden.
Why Professional Assessment Matters
Many people spend months or even years trying home remedies without success, simply because they are treating a different type of fungal infection.
Successful treatment begins with identifying exactly where the fungus is located, whether it is on the surface of the nail, beneath the nail plate, or involving the nail root.
Once the type and stage of the infection have been identified, the most appropriate treatment plan can be chosen, giving the best opportunity for healthy, fungus-free nail growth.
For more information or to book an appointment please call our clinic +971 4 3435390 or WhatsApp +971 50 3553024



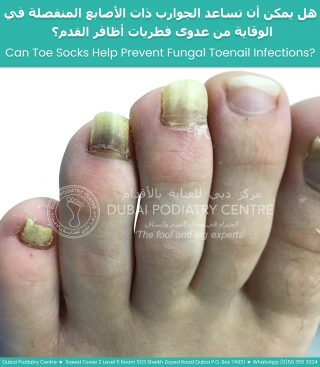 When the toes are squeezed together for long periods, moisture becomes trapped and air circulation is reduced. This creates the perfect environment for fungal spores to grow and spread. Over time, the infection may remain confined to the skin between the toes, or it may spread into the neighbouring toenails, particularly the fourth and fifth toenails, resulting in fungal nail infection (onychomycosis).
When the toes are squeezed together for long periods, moisture becomes trapped and air circulation is reduced. This creates the perfect environment for fungal spores to grow and spread. Over time, the infection may remain confined to the skin between the toes, or it may spread into the neighbouring toenails, particularly the fourth and fifth toenails, resulting in fungal nail infection (onychomycosis).

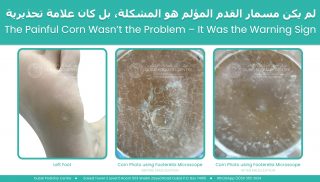
 The condition is caused by a virus that is spread through contact with infected skin cells. This typically occurs in high-risk environments where people walk barefoot, such as swimming pools, gym changing rooms, and water parks. An infected skin cell from another person can be shed onto the floor, and if you walk over that area within a short time frame, the virus may transfer to your foot.
The condition is caused by a virus that is spread through contact with infected skin cells. This typically occurs in high-risk environments where people walk barefoot, such as swimming pools, gym changing rooms, and water parks. An infected skin cell from another person can be shed onto the floor, and if you walk over that area within a short time frame, the virus may transfer to your foot. Plantar warts are sometimes confused with corns, but they are very different. A corn is a build-up of hard skin caused by pressure and friction. It can often be reduced without bleeding, although it may feel like walking on a sharp point. A plantar wart, however, is a living viral lesion. If disturbed or cut, it will bleed because it has developed its own blood supply within the skin.
Plantar warts are sometimes confused with corns, but they are very different. A corn is a build-up of hard skin caused by pressure and friction. It can often be reduced without bleeding, although it may feel like walking on a sharp point. A plantar wart, however, is a living viral lesion. If disturbed or cut, it will bleed because it has developed its own blood supply within the skin.