At Dubai Podiatry Centre, we sometimes see teenagers whose toenails look damaged, rough or uneven, but when we examine the nail closely, there is actually nothing wrong with the health of the nail itself.
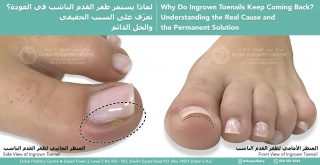
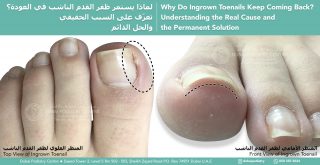
Recently, a mother brought her teenager to see us because they were repeatedly peeling both their fingernails and toenails. The toenails had been peeled so frequently that they had developed sharp and rough edges, with some edges beginning to irritate the surrounding skin and contribute to ingrown toenails.
However, when we examined the feet, the underlying picture was very reassuring.
The nails were growing extremely well from the nail root and nail bed. The skin underneath was healthy and pink, and the circulation and capillary refill were excellent.
The problem was not that the toenails were unhealthy.
The problem was the repeated picking and peeling of perfectly healthy nails.
Why Do Some Teenagers Pick Their Nails Without Realising It?
The teenager’s mother explained that the picking was almost constant, particularly while studying, concentrating or thinking.
Interestingly, the teenager was often not consciously aware that they were doing it.
This is an important distinction. Sometimes repetitive nail picking is less about the nail itself and more about giving the hands something to do while the brain is concentrating.
Some children and teenagers naturally seek movement or tactile stimulation when focusing. Their fingers want to touch, roll, pick or manipulate something while their attention is occupied elsewhere.
If there is nothing else available, the fingernails, skin or toenails can become the target.
Nail Polish Isn’t Necessarily the Answer
Parents understandably ask whether we can put something onto the nail to stop the behaviour.
- Would a special nail polish help?
- Would a strengthening lacquer help?
- Does the nail need a treatment?
If the nail itself is healthy, coating it does not necessarily address the reason the picking is happening.
From a podiatry perspective, our priority is to examine the nail carefully and establish whether there is an underlying nail or skin condition. We can also safely smooth or treat damaged edges and manage an ingrown toenail if repeated peeling has created a sharp nail spike.
But when the nail is healthy and the damage is being caused by repeated picking, it is also important to address the habit itself.
Give the Fingers Something Else to Do
One of the simplest strategies can be to redirect the hands towards something harmless.
A small piece of therapy putty, reusable putty, Blu Tack or Play-Doh can be surprisingly useful.
While studying, reading, watching television or concentrating, the teenager can gently roll and manipulate the putty between their fingers.
The objective isn’t simply to say: “Stop picking your nails.”
Instead, we are giving the fingers an alternative activity.
This can be particularly useful because it is quiet and discreet. The teenager can manipulate a small piece of putty underneath a desk or while reading without disturbing the people around them.
Fidget spinners and other sensory devices can also be helpful for some people. However, they can sometimes become visually or audibly distracting to classmates, siblings or other people nearby. A small piece of putty can provide tactile stimulation much more discreetly.
Keeping Busy Hands Away From Healthy Nails
Some teenagers who enjoy using their hands are wonderful at detailed activities. They may enjoy drawing, crafts, model making, painting miniatures or other projects requiring very delicate hand movements.
Those activities are excellent when there is time to concentrate on the activity itself.
The difficulty comes when the teenager needs their attention elsewhere, particularly during studying.
That is when a very simple tactile object can be useful. The hands can remain gently occupied while the brain concentrates on the information being learned.
Protecting the Toenails While the Habit Changes
While working on reducing the picking habit, it is important to protect the toenails from secondary problems.
Repeatedly peeling a toenail can leave:
- Sharp or jagged nail edges
- Very short nails
- Irritated skin around the nail
- Nail edges that begin to grow into the surrounding skin
- Tenderness or inflammation
- Increased risk of breaking the skin
If an edge has become sharp, painful or ingrown, a podiatrist can examine and manage it appropriately.
It is also important not to assume that every damaged-looking nail is caused by picking. Fungal infections, trauma, skin conditions and other nail disorders can alter the appearance of toenails, so an examination can be helpful when the cause isn’t clear.
When Should Parents Seek Further Advice?
Occasional nail picking can simply be a habit. However, if the behaviour is frequent, difficult for the young person to control, causes bleeding or significant tissue damage, causes distress, or begins to interfere with everyday life, parents may wish to discuss it with their GP, paediatrician or an appropriate behavioural or mental-health professional.
The important thing is not to shame the teenager for doing something they may barely realise they are doing.
Sometimes the first useful question isn’t: “How do we make them stop?”
It is: “What can we give their hands to do instead?”
At Dubai Podiatry Centre, we can assess toenails that have become painful, rough or ingrown as a result of repeated picking and determine whether the nail itself is healthy or whether another nail condition requires treatment.
Dubai Podiatry Centre
Helping to keep growing feet and toenails healthy.
For more information or to book an appointment please call our clinic +971 4 3435390 or WhatsApp +971 50 3553024