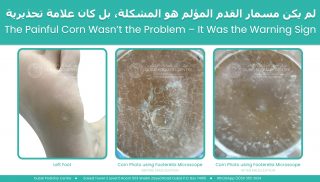
A patient attended our clinic today complaining of severe pain underneath the outside of his left foot. The pain had become so intense that he was limping and described the sensation as walking on a sharp piece of glass.
On examination, we found a hard corn underneath the fifth metatarsal head on the outside border of his left foot. Many people assume that a corn is the problem, but in reality a corn is often the body’s attempt to protect itself from excessive pressure.
We removed the corn painlessly, and the patient experienced immediate relief. However, we explained that unless we addressed the underlying cause, the corn would simply return.
To investigate further, we performed a 3D body scan and biomechanical assessment.
The results were fascinating.
The patient had a significant imbalance throughout his body. His left leg was functionally longer than his right. His pelvis was tilted, with the right side anteriorly tilted and the left side posteriorly tilted. He was carrying considerably more body weight through the left side of his body, creating excessive pressure beneath the outside of the left foot.
His medical history helped explain the pattern. He had previously undergone two lower back surgeries on the left side, suffered left hip problems, torn ACL injuries involving the left knee, and undergone left Achilles tendon surgery.
Over many years, his body had adapted to these injuries.
The scan showed that his pelvis had shifted towards the left side, causing increased loading through the left leg and foot. At the same time, his right foot was internally rotated and functioning almost like a golfer at the top of a backswing position. This created high tensile stress through the right Achilles tendon, the right knee, and the lower back while simultaneously increasing compression forces through the left side of the body.
The painful corn underneath the left foot was simply the area where the body was absorbing the greatest amount of pressure.
The development of a corn follows a predictable sequence.
First, the body produces a layer of hard skin to protect itself. This creates a broad plaque of callus, similar to a pancake of thicker skin.
If the pressure continues, the body creates a concentrated plug of dense keratin at the centre of the pressure point. Keratin is the same material found in toenails. This hard central core forms what we recognise as a hard corn.
As pressure continues to increase, inflammation develops beneath the area. Patients often describe burning, stinging, or sharp sensations. This was the stage our patient had reached.
If left untreated, the next stage can be the formation of a soft corn. The tissues become saturated with inflammatory fluid and appear white, rubbery, and extremely painful.
The final stage is tissue breakdown and ulceration.
This progression is particularly important in patients with diabetes, neuropathy, or vascular disease. These patients may not feel the early warning signs of pressure and pain. As a result, the protective stages can progress unnoticed until an ulcer develops.
Many patients believe ulcers appear suddenly and without warning. In reality, the body often gives multiple warning signals beforehand, but if sensation is reduced, those signals may not be recognised.
For this patient, the solution was not repeated corn removal.
The solution was correcting the forces causing the corn.
We prescribed custom corrective orthotics designed specifically for his individual biomechanics. The right orthotic was intentionally very different from the left because each side of the body required a different correction.
The aim was to improve pelvic balance, reduce the functional leg length discrepancy, redistribute pressure more evenly between both feet, and decrease excessive loading through the left foot.
We performed further scans with the orthotics in place and saw immediate improvements in alignment and pressure distribution.
The body can be compared to a wobbly table. If one table leg is shorter than the others, the tabletop becomes uneven. Placing a carefully measured support beneath the shorter leg restores balance.
Corrective orthotics work in a similar way. While we cannot make one leg physically grow longer, we can improve balance and alignment so that the body functions more efficiently and with less stress.
The patient will return in three months for reassessment. As the body adapts to improved alignment, muscle tension, posture, and weight distribution can all change. Repeat scanning will allow us to monitor these changes and determine whether further orthotic adjustments are required.
The important lesson from this case is that a corn is rarely just a skin problem.
A corn is often a warning sign that excessive pressure is travelling through a specific part of the foot. Removing the corn may provide temporary relief, but identifying and correcting the underlying mechanical cause is what provides a long-term solution.
For more information or to book an appointment please call our clinic +971 4 3435390 or WhatsApp +971 50 3553024

 The condition is caused by a virus that is spread through contact with infected skin cells. This typically occurs in high-risk environments where people walk barefoot, such as swimming pools, gym changing rooms, and water parks. An infected skin cell from another person can be shed onto the floor, and if you walk over that area within a short time frame, the virus may transfer to your foot.
The condition is caused by a virus that is spread through contact with infected skin cells. This typically occurs in high-risk environments where people walk barefoot, such as swimming pools, gym changing rooms, and water parks. An infected skin cell from another person can be shed onto the floor, and if you walk over that area within a short time frame, the virus may transfer to your foot. Plantar warts are sometimes confused with corns, but they are very different. A corn is a build-up of hard skin caused by pressure and friction. It can often be reduced without bleeding, although it may feel like walking on a sharp point. A plantar wart, however, is a living viral lesion. If disturbed or cut, it will bleed because it has developed its own blood supply within the skin.
Plantar warts are sometimes confused with corns, but they are very different. A corn is a build-up of hard skin caused by pressure and friction. It can often be reduced without bleeding, although it may feel like walking on a sharp point. A plantar wart, however, is a living viral lesion. If disturbed or cut, it will bleed because it has developed its own blood supply within the skin.