Written by Michelle Champlin BSc Pod., M.Ch.S., S.R., Ch., (UK)
Your feet don’t have just one arch, but three. They work together to create arches or ‘caves’ that create stability, provide flexibility and shock absorption and also propulsion to move you forward. Chief Podiatrist Michelle Champlin explains what the transverse arch does and how its collapse can create a range of foot-related issues.
Mrs Champlin explains “The foot shows up your general health – as the furthest from your heart, sensory and nerve problems show up first in the feet. This is the main reason why diabetics come for an annual or bi-annual foot check with the Podiatrist, to catch any impairment early before it affects major organs. There are three arches of your feet – the main one we all know of on the inside of your foot, and also one on the outside of the foot. The most important one in my opinion is an arch running across the front of the foot – the transverse arch. If this collapses, then the other two collapse in turn.”
The arches in your foot provide structural support, like a cave or bridge
The transverse arch is in your forefoot and ‘depth-wise’ runs from the metatarsal heads back to the tarsal bones, and across the foot from the inside to the outside edges of the foot. At the forward aspect of the transverse arch, the metatarsal heads contact the ground. Collapse of the transverse arch will often result in a build-up of thick callous underneath the metatarsal heads. Left untreated, “dropped” metatarsal heads and/or irritation of one of the interdigital nerves (a “Morton’s neuroma”) is also a good indications that this arch is not being supported properly by the plantar fascia, the thick band of tissue connecting your heelbone to your forefoot. In turn, constant pulling on the fascia can lead to heel pain, or ‘plantar fasciitis’.
Collapse of the transverse arch can also lead to the forefoot splaying and spreading out, resulting in bunions or bunionettes.
Collapse or dysfunction of any of the foot’s three arches needs to be addressed by your Podiatrist, specializing in biomechanics, with custom-made stabilizing orthotics that will support the foot both when standing and throughout the gait cycle, while controlling the impact forces. Orthotics can also be custom designed for the different movements and forices specific to certain sports, from football to skiing. Particularly when there is asymmetry between the feet or legs, arch problems can cause abnormal rotational forces to be transmitted through the ankles, leg bones, knee joints and into the pelvis and spine, resulting even in hip or lower back pain.
If you are experiencing foot, ankle, leg or hip pain, contact the podiatry team at Dubai Podiatry Centre on +971 4 3435390.
بقلم ميشيل شامبلين
لا تحتوي قدميك على قوس واحد فقط، بل ثلاثة. إنهم يعملون معًا لإنشاء أقواس أو “كهوف” توفر الاستقرار وتوفر المرونة وامتصاص الصدمات وأيضًا الدفع للمضي قدمًا. تشرح رئيسة أطباء الأقدام ميشيل شامبلين ما يفعله القوس المستعرض وكيف يمكن أن يؤدي انهياره إلى خلق مجموعة من المشكلات المتعلقة بالقدم.
تشرح السيدة شامبلن أن “القدم تظهر صحتك العامة – فبما أن المشاكل الحسية والعصبية تظهر أولاً في القدمين، فكلما كان أبعد عن قلبك. وهذا هو السبب الرئيسي الذي يدفع مرضى السكر إلى مراجعة قدمهم بشكل سنوي أو نصف سنوي لدى طبيب الأقدام، لاكتشاف أي ضعف مبكرًا قبل أن يؤثر على الأعضاء الرئيسية. هناك ثلاثة أقواس لقدميك – القوس الرئيسي الذي نعرفه جميعًا موجود في الجزء الداخلي من قدمك، وأيضًا القوس الموجود في الجزء الخارجي من القدم. وأهمها في رأيي هو القوس الذي يمتد عبر مقدمة القدم – القوس المستعرض. إذا انهار هذا، فإن الاثنين الآخرين ينهاران بدورهما.
توفر الأقواس الموجودة في قدمك الدعم الهيكلي، مثل الكهف أو الجسر
يوجد القوس المستعرض في مقدمة قدمك ويمتد “بعمق” من رؤوس مشط القدم إلى عظام الكاحل، وعبر القدم من الداخل إلى الحواف الخارجية للقدم. في الجانب الأمامي من القوس المستعرض، تلامس رؤوس مشط القدم الأرض. غالبًا ما يؤدي انهيار القوس المستعرض إلى تراكم مادة قاسية سميكة أسفل رؤوس مشط القدم. إن ترك رؤوس مشط القدم “المسقطة” دون علاج و/أو تهيج أحد الأعصاب بين الأصابع (“ورم مورتون العصبي”) يعد أيضًا مؤشرًا جيدًا على أن هذا القوس لا يتم دعمه بشكل صحيح بواسطة اللفافة الأخمصية، وهو شريط سميك من الأنسجة يربط بين قدميك. عظم الكعب إلى مقدمة قدمك. وفي المقابل، يمكن أن يؤدي الشد المستمر على اللفافة إلى ألم في الكعب، أو “التهاب اللفافة الأخمصية”.
يمكن أن يؤدي انهيار القوس المستعرض أيضًا إلى تباعد مقدمة القدم وانتشارها، مما يؤدي إلى ظهور أورام أو أورام.
يجب معالجة الانهيار أو الخلل الوظيفي في أي من أقواس القدم الثلاثة بواسطة طبيب الأقدام الخاص بك، المتخصص في الميكانيكا الحيوية، باستخدام أجهزة تقويم العظام المصممة خصيصًا والتي ستدعم القدم أثناء الوقوف وطوال دورة المشي، مع التحكم في قوى التأثير. يمكن أيضًا تصميم أجهزة تقويم العظام خصيصًا لمختلف الحركات والقوى الخاصة برياضات معينة، من كرة القدم إلى التزلج. خاصة عندما يكون هناك عدم تناسق بين القدمين أو الساقين، يمكن أن تتسبب مشاكل القوس في انتقال قوى دوران غير طبيعية عبر الكاحلين وعظام الساق ومفاصل الركبة إلى الحوض والعمود الفقري، مما يؤدي حتى إلى آلام الورك أو أسفل الظهر.
إذا كنت تعاني من آلام في القدم أو الكاحل أو الساق أو الورك، اتصل مركز دبي لعلاج الأقدام على الرقم 043435390.
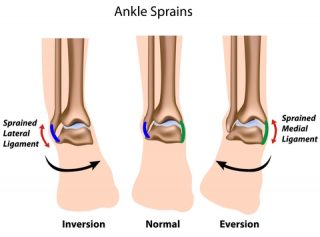 The deltoid ligament (also called the medial ligament) is a strong band that connects your lower leg bone (tibia) to the inner side of your ankle (also called the ‘medial’ side of your ankle). This triangular shaped ligament supports your ankle and prevents it from over rotating to the outer side. Strong, connective fibrous band, it is one of the strongest structures in the body.
The deltoid ligament (also called the medial ligament) is a strong band that connects your lower leg bone (tibia) to the inner side of your ankle (also called the ‘medial’ side of your ankle). This triangular shaped ligament supports your ankle and prevents it from over rotating to the outer side. Strong, connective fibrous band, it is one of the strongest structures in the body.