Chief Podiatrist Michelle Champlin of Dubai Podiatry Centre shares her advice on pedicures, polish and toenail health. Is it bad to keep nail polish on for weeks?
What are the main issues that people come to Dubai Podiatry Centre for?
We see men, women and children in equal numbers. Anyone who’s got a pair of feet comes to the clinic and can need a podiatrist for one problem or another. For women, we see a lot of toenail issues – partly because it’s so accessible here to have pedicures. We see a lot of problems with toenails and fungal infections. Men – a lot of sports injuries and for children, we see a high number of sports injuries and ‘flat feet’. Children in Dubai are so sporty (which is fabulous), and we see them doing sports every single day, instead of when I was a child we would do sports maybe for an hour once a week. Children now are getting sports injuries from the amount of sports that some of them are playing – everything from ankle sprains to verrucas caught at the swimming pool or foot pain linked with flat feet. We want people to be active – but it’s about taking care of yourself too, and we’re here to get people back being active with minimal down time.
Fungal infections and toenails – why is this linked to having pedicures?
You can have a pedicure without having nail polish applied. It’s called an ‘essential pedicure’. Or you can go for a medical pedicure with a Podiatrist. Because toes and feet are being exposed much of the time with sandals here in Dubai, we’re seeing nails being painted much more. When nails are painted, the nail plate is porous so it can absorb liquid. It can also excrete liquid as well. We sweat through our nail beds and it comes out through the nail – that’s what makes the nail flexible. But if you cover it with nail polish, you’re putting a waterproof nail lacquer on the top of it and fungus can then breed underneath.
So nail polish traps the fungus?
Yes – everybody has fungus all over their bodies – it’s normal. But if you coat the nail plate with a base coat, two colour coats, and then a top coat to keep it shiny and make it last longer, there is absolutely no moisture coming through the nail plate and into the atmosphere, so it gets stuck underneath. And if you’re changing your nail polish every week, it’s only off for half an hour during the process. Removing the nail polish, pedicuring and then reapplying it, your nail polish is essentially on for the entire year. The one time you take it off, and your nail’s gone all white underneath, or green or another colour of the rainbow. A Podiatrist can treat the fungal nail infection to get your nails healthy again – you can also read my tips on home care of fungal toenails.
So what should a healthy toenail look like?
A healthy toenail is more or less clear with a very slight yellow tinge to it because of the keratin that’s in the nail. It depends on the health of the nail bed, which is the skin underneath – you can check out our recent blog as well on nail colours and what they can mean. So if you’re a heavy smoker, then the nail bed will be slightly grey-blue in appearance and the nail will grow thicker and look a bit more yellow. If you’re a healthy person, your nail will be 1.5mm thick and will grow so that you need to trim it every 1-2 weeks. So it should have a light pinkish appearance due to the nail bed underneath and with a very slight tint of yellow from the keratin.
Worried about a change in your toenail colour, an ingrowing nail, or foot pain? Contact the team at Dubai Podiatry Centre, led by Chief Podiatrist Michelle Champlin on +971 4 3435390 for expert, friendly foot care.
تشاركنا ميشيل شامبلين، رئيسة أطباء الأقدام في مركز دبي لعلاج الأقدام، نصائحها بشأن العناية بالأقدام، وتلميع الأظافر، وصحة أظافر القدمين. هل من السيء إبقاء طلاء الأظافر لأسابيع؟
ما هي القضايا الرئيسية التي يأتي الناس إلى مركز دبي لعلاج الأرجل بسببها؟
نرى الرجال والنساء والأطفال بأعداد متساوية. أي شخص لديه قدمين يأتي إلى العيادة ويمكن أن يحتاج إلى طبيب أقدام لمشكلة أو أخرى. بالنسبة للنساء، نرى الكثير من المشكلات المتعلقة بأظافر القدمين – ويرجع ذلك جزئيًا إلى إمكانية الوصول إلى خدمات العناية بالأقدام هنا. نرى الكثير من المشاكل مع أظافر القدمين والالتهابات الفطرية. الرجال – هناك الكثير من الإصابات الرياضية، وبالنسبة للأطفال، نرى عددًا كبيرًا من الإصابات الرياضية و”الأقدام المسطحة”. الأطفال في دبي رياضيون للغاية (وهو أمر رائع)، ونراهم يمارسون الرياضة كل يوم، فبدلاً من عندما كنت طفلاً كنا نمارس الرياضة ربما لمدة ساعة مرة واحدة في الأسبوع. يتعرض الأطفال الآن لإصابات رياضية بسبب كمية الألعاب الرياضية التي يمارسها بعضهم – كل شيء بدءًا من الالتواء في الكاحل إلى الثآليل التي تحدث في حمام السباحة أو آلام القدم المرتبطة بالأقدام المسطحة. نريد أن يكون الأشخاص نشطين – ولكن الأمر يتعلق بالعناية بنفسك أيضًا، ونحن هنا لإعادة الأشخاص إلى نشاطهم بأقل وقت من التوقف.
الالتهابات الفطرية وأظافر القدمين – لماذا يرتبط ذلك بالباديكير؟
يمكنك الحصول على باديكير دون الحاجة إلى تطبيق طلاء الأظافر. يطلق عليه “الباديكير الأساسي”. أو يمكنك الذهاب للحصول على باديكير طبي مع طبيب الأقدام. نظرًا لأن أصابع القدمين والقدمين تكون مكشوفة معظم الوقت عند ارتداء الصنادل هنا في دبي، فإننا نشهد طلاء الأظافر بشكل أكبر بكثير. عندما يتم طلاء الأظافر، تكون صفيحة الظفر مسامية حتى تتمكن من امتصاص السائل. ويمكنه أيضًا إخراج السوائل أيضًا. نحن نتعرق من خلال أظافرنا ويخرج من خلال الظفر، وهذا ما يجعل الظفر مرنًا. ولكن إذا قمت بتغطيتها بطلاء أظافر، فإنك تضع طلاء أظافر مقاوم للماء فوقها ويمكن للفطريات أن تتكاثر تحتها.
طلاء الأظافر يحبس الفطريات؟
نعم، يعاني الجميع من الفطريات في جميع أنحاء أجسادهم، وهذا أمر طبيعي. ولكن إذا قمت بتغطية صفيحة الظفر بطبقة أساسية، وطبقتين ملونتين، ثم طبقة علوية للحفاظ على لمعانها وجعلها تدوم لفترة أطول، فلن يكون هناك أي رطوبة على الإطلاق تدخل عبر صفيحة الظفر إلى الغلاف الجوي، وبالتالي تلتصق تحته. وإذا كنت تقومين بتغيير طلاء أظافرك كل أسبوع، فلن يتم تغييره إلا لمدة نصف ساعة خلال هذه العملية. إزالة طلاء الأظافر، والباديكير ثم إعادة تطبيقه، سيظل طلاء أظافرك ثابتًا طوال العام. بمجرد خلعه، يصبح ظفرك أبيض بالكامل من تحته، أو أخضر أو أي لون آخر من ألوان قوس قزح. يمكن لطبيب الأقدام علاج عدوى الأظافر الفطرية لاستعادة صحة أظافرك مرة أخرى – يمكنك أيضًا قراءة نصائحي حول الرعاية المنزلية لأظافر القدم الفطرية.
إذًا كيف ينبغي أن تبدو أظافر القدم الصحية؟
يكون أظافر القدم الصحي أكثر أو أقل وضوحًا مع مسحة صفراء طفيفة جدًا بسبب الكيراتين الموجود في الظفر. يعتمد ذلك على صحة طبقة الظفر، وهو الجلد الموجود تحتها – يمكنك الاطلاع على مدونتنا الحديثة أيضًا حول ألوان الأظافر وما يمكن أن تعنيه. لذا، إذا كنت من المدخنات الشرهات، فسيكون مظهر سطح الظفر رماديًا مزرقًا قليلًا وسينمو الظفر أكثر سمكًا وسيبدو أصفر أكثر قليلًا. إذا كنت شخصًا يتمتع بصحة جيدة، فسيكون سمك ظفرك 1.5 ملم وسينمو بحيث تحتاج إلى تقليمه كل أسبوع أو أسبوعين. لذلك ينبغي أن يكون له مظهر وردي فاتح بسبب طبقة الظفر الموجودة أسفله مع صبغة خفيفة جدًا من اللون الأصفر من الكيراتين.
هل تشعر بالقلق من تغير لون أظافر قدميك أو ظهور ظفر نام أو ألم في القدم؟ اتصل بفريق مركز دبي لعلاج الأقدام، بقيادة رئيسة أطباء الأقدام ميشيل شامبلين على الرقم 043435390 للحصول على رعاية احترافية وودية للقدمين.
 Written by Michelle Champlin BSc Pod., M.Ch.S., S.R., Ch., (UK)
Written by Michelle Champlin BSc Pod., M.Ch.S., S.R., Ch., (UK)



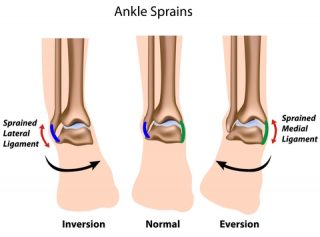 The deltoid ligament (also called the medial ligament) is a strong band that connects your lower leg bone (tibia) to the inner side of your ankle (also called the ‘medial’ side of your ankle). This triangular shaped ligament supports your ankle and prevents it from over rotating to the outer side. Strong, connective fibrous band, it is one of the strongest structures in the body.
The deltoid ligament (also called the medial ligament) is a strong band that connects your lower leg bone (tibia) to the inner side of your ankle (also called the ‘medial’ side of your ankle). This triangular shaped ligament supports your ankle and prevents it from over rotating to the outer side. Strong, connective fibrous band, it is one of the strongest structures in the body.